
Testimony and comments spread misinformation and divert from meaningful improvement

- You can email your legislators here
HB 1472 is a straightforward bill: it consolidates institutional settings for people with intellectual and other developmental disabilities (IDD) from four sites to two. It was requested by the state Office of Financial Managment and is a part of a decades-long effort to reduce our institutional footprint while expanding care options for all.
- It does not take away services.
- It does not end institutional care for people with IDD.
- The type of services affected would continue at Fircrest near Seattle, and Lakeland Village near Spokane, and they have capacity.
- It also does not remove overnight respite options.
It consolidates one intermediate care facility and one nursing home into existing ones in Fircrest near Seattle and Lakeland Village near Spokane. The two remaining institutions would each offer both types of facilities. All residents at Rainier and Yakima Village would have a choice to continue with institutional care or move to a community setting.
And yes – the state and IDD community DO have quite of bit of experience helping people transition out of institutions, safely.
Community options for IDD services need more support. We all know this. But the fixes are achievable IF legislators choose to support them.
Fearmongering
In testimony and legislative debate, we have heard several points that are not substantiated by facts and that ignore the transformation of service delivery since the 1970s.
The most alarming is that people will die – one legislator suggested hundreds, even though only about 100 people will be affected by the consolidation.
Another suggested we have no community infrastructure to support people with IDD and that we have no plan or way to transition people to other settings, even similar ones.
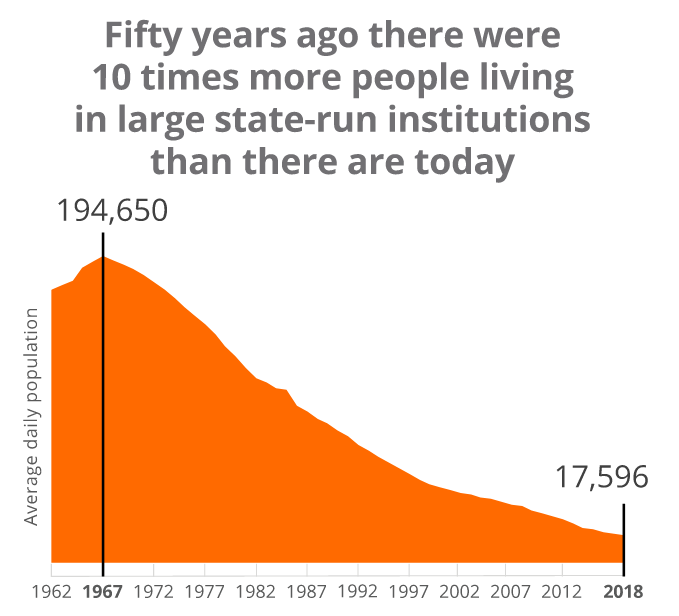
THE TRUTH: People have been moving out of our state institutions for decades, safely. We have downsized successfully - we did it gradually over decades.
Since the 1970s, we successfully shifted from serving 4,000 to 5,000 adults and children in institutional settings, to serving 65,000 in the community.
For people requiring residential care, our statewide system of Supported Living providers serves 4,500 adults. Hundreds of others live in adult family homes, companion homes, and assisted living facilities. Even more live with family members.
Challenges
Do we need to better invest and refine some community services? Absolutely.
There is a pilot program for Supported Living community residential that combines training in behavior support with additional pay that has resulted in safe placements for people with complex behavior.
Another program improved community connection for people living in adult family homes.
Families have championed community day respite for years – and plead for more access.
THE TRUTH: People speaking out against HB 1472 are not suggesting expanding on success. They are not talking about serving more people, or all folks better. Or addressing the issues that prevent people from fully accessing support.
They are saying people with IDD living in institutions cannot leave without jeopardizing their health. Once in, you can’t check out.
And that is a dangerous lie.
Today, people with IDD live longer, healthier lives BECAUSE they are able access care and services in their communities. All relevant research supports the fact that community settings result in improved quality of life in areas of integration, social participation, employment, choice-making and self-determination, quality and duration of services, contact with friends and relatives, and other indicators.
This bill does not require anyone to move into
the community. And it doesn't shift large numbers into the other institutions, also called residential habilitation centers, or RHCs for short. Based on past consolidations and waiting lists of people who have already requested community care, DSHS expects half of the 120 or so to move to community settings and half to move to either Fircrest or Lakeland Village.
Fundamentally, the question is: Do we still need four institutions?
From 1,900 residents to 71
At Rainier School, one of the sites that would close, enrollment declined from a peak of 1,900 in the late 1950s, to 318 in 2018, to 71 today.
Rainier opened in 1939 and operates something called an intermediate care facility for people with intellectual disabilities (ICF/ID). These are transitional programs where adults with cognitive disabilities that started in childhood go to receive “active treatment” in adaptive skill development.
Yakima Valley, the other site subject to closure, opened in the 1950s and began as an institution for children with intellectual disabilities. After public schools were required to serve children with IDD, Yakima converted to a nursing home. Today, about 30 adults with IDD live in an aging facility built to serve hundreds.
If HB 1472 passes, residents at Rainer and Yakima Valley retain the right of choice.
The 71 residents at Rainier will be able to choose a community residential option – such as Supported Living and related services – or transfer to an ICF/ID at either Fircrest or Lakeland Village.
The 30 residents at Yakima Valley can choose a community option, such as an adult family home or assisted living facility, or one of the IDD nursing facilities at Fircrest or Lakeland Village.
The overnight, short-term respite at Yakima would continue. Those services are available for up to 30 days for eligible DDA clients.
Transition support – and years of practice
People opposed to the bill have also suggested that folks would be left adrift – cut off from service or care. Or that the state lacked ability or structure to help with transitions.
THE TRUTH: When people with IDD transition to community services, they have extensive, individualized support from family mentors who explain options, assist with decision-making, and ensure everything is in place before a move. Their work is personal, hands-on, and rooted in lived experience. You can read some of their success stories here.
Individuals moving have access to the PATH Program of peer mentors.
Roads to Community Living covers the first year of transition to the community, and involves careful, individualized planning and person-centered coordination to ensure success. That program has been around since 2007.
DSHS also has years of experience to draw from, including four times when dozens at a time needed support moving to new care facilities or community placements. The most recent was in 2022. The moves:
1994 - Interlake School in Medical Lake closed. It served 150 people with IDD who were considered medically fragile. All transitioned to community settings or another institution.
2002 - After the Olmstead decision affirmed the right to community services, the state budgeted to assist 80 people to transition out of institutions; 61 took up the offer and successfully moved out – including people with high support needs and complex behavior.
2011 - The Frances Haddon Morgan Center closed, prompting transitions for 52 residents. In the months before closure, 2 suspicious deaths were investigated at the facility. After leaving, one person died after drinking laundry detergent, but multiple investigations determined the move was not directly responsible. The state did a follow-up report a year later and found all other former residents were stable in their new settings. Some insights from that report:
- Anxiety resolved most quickly for those who chose Supported Living community residential.
- Challenging behaviors for most improved or stayed the same.
- Those who chose community settings were more likely to have friends, visit people they cared about, and have friends visit them.
- A year in, all families and guardians said they were confident the participant was safe in their new home.
- Numerous families “noticed their family members seem to be happier.”
2022 – Most recently, the state closed part of Rainier School after it was de-certified and federal funds were pulled. From 2022 to 2023, 57 residents transitioned out. Again, they were given the choice of a community placement or transfer to another institutional setting, and support during and after the transition.
This isn't to say transitions are easy. But we do have experience. In 2022, DSHS developed a process guide, quality framework, a heightened review protocol, and a transition stabilization protocol. During the transition, staff continued to be available to spend time in the new resident’s home after the move, and family mentors with lived experience continued to offer crucial resources to families and guardians of those leaving, including helping them understand the process and learn about community supports available.
Stability is a critical care component for many – whether they live and receive support in an institution or in a community setting. But we can mitigate, we can plan, and we can pace the transition.
Build the future
The Arc supports community. This is no secret. We are driven by the fundamental belief that everyone deserves to write their own life story. That means:
- Real access to education
- Meaningful employment
- Quality healthcare
- Genuine community connections
Some comments heard in hearings, executive sessions, and floor speeches disregard the tremendous work of thousands of people with IDD, their family members, and professionals to make community inclusive.
We DO have a network of community services, and we need legislators to learn about it, invest in it, and help us address and improve the gaps.
This quote from a 2003 state report stands out:
“At this point it is generally accepted that with very few exceptions, any person who lives in an RHC can live safely and well in the community, given the funding necessary to provide the supports needed.”
That same report found that the main barriers to phasing out institutions are NOT that people are too fragile to leave.
The barriers are:
- Lack of affordable and accessible housing for people with extremely low, fixed incomes
- Limited services available to people with challenging support needs or complex health
Those are solvable. Legislators have responded to the first, and we need them to engage - with urgency - on the second.
In the last two years they have put close to $50 million into IDD housing. In the next two-year capital budget, they are proposing up to $55 million for IDD housing. This can be used for new construction or renovation.
For the second challenge, legislators need to stay focused, invest strategically, and keep the promise: Improve and expand community options so we can all thrive.
- Written by Ramona Hattendorf, Director of Public Policy and Civic Engagement at The Arc of King County
.png)
{kind=link}